
bestbrk/istock via Getty Images
Understanding 2021 Changes in Emergency Medicine Reimbursement
From surprise billing legislation to Medicare payment updates, emergency medicine reimbursement will face key changes in 2021 that will impact provider revenue.
Emergency medicine groups face several changes this year, including a new federal ban on surprise medical billing, updates to the Medicare reimbursement formula, changes to the CMS MIPS program, and new billable services. Below is a summary of these changes provided by the experts at Brault Practice Solutions.
Federal Ban on Surprise Medical Billing
At the end of 2020, Congress passed a major omnibus bill that included a federal ban on surprise medical billing (SMB) called the “No Surprises Act.” This legislation resulted after years of discussion with both physician groups and insurance providers. Both sides agreed that patients should be removed from what is essentially a payment dispute. However, there was a lot of debate on how to approach this on such a large scale and with concern for unanticipated consequences.
“The federal ban on surprise billing was long overdue,” explains Dr. Andrea Brault, President and CEO of Brault Practice Solutions and advocate for independent physician practices. “Many states have already moved in this direction, but these state laws didn’t always address the ERISA plans that now makeup the majority of individual, employer-based health plans. So, the result was public frustration and more confusion.”
Dr. Brault explains that it was really up to federal lawmakers to establish a uniform set of rules that would address the ERISA plans and also address those states without comprehensive patient protections for out-of-network care.
She explains how the medical provider community spent a lot of time educating lawmakers about the potential effects of these new rules and, in some areas, they were able to impart some reasonable guidance, including:
- Requiring timely responses from insurers (must pay or deny within 30 days)
- Creating an Independent Dispute Resolution process, with no minimum threshold to access mediation (including high-volume, low-dollar disputes that makeup the majority of ED claims)
- Allowing similar claims to be batched for added efficiency
- Requiring mediators to consider prior contracted rates, and prohibiting them from comparing those rates to public payer rates (which are designed to be lower than commercial rates)
However, Dr. Brault explains that the new federal SMB law also includes some requirements that will create new challenges for those in emergency medicine. For example:
- Limits on claim batching (only within a 30-day period)
- A 90-day “cooling off period” before a new dispute can be made (which will significantly delay timely, appropriate payment on the majority of disputed claims)
- Early language that indicates batching will only be allowed for same Provider or same Facility (despite ED services being billed by TINs)
- Requiring mediators to consider the plan’s median in-network rate, but prohibiting them from comparing those rates to billed charges or usual and customary rates.
“We now have the rest of the year to prepare for these changes, before the new law goes into effect in 2022,” explains Dr. Brault. “Hospital-based physician groups should be reaching out to their advocacy organizations for opportunities to participate in the rule-making or administrative phase as they are the most likely to be impacted by this Act. The negative or positive impacts of this new law will depend on the details to be hammered out in 2021.”
An increase in RVUs for emergency department E/M codes
In 2021, emergency medicine providers will also see changes related to the Final Rule of the Medicare Physician Fee Schedule (PFS) – including an increase in Relative Value Units (RVUs) for Emergency Department (ED) evaluation and management (E/M) codes 99283-99285.
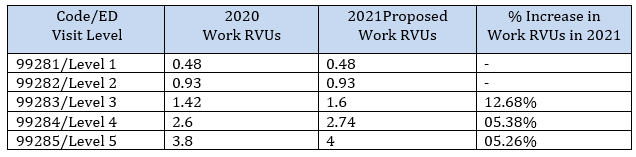
“This is an important update for emergency groups to be aware of,” explains Dr. Brault. “This increase in RVUs applies directly to Medicare reimbursement, but it’s worth noting that many commercial payers also consider these values in their formulas for reimbursement. So, keep an eye on your payments/RVU (by Payer) and be aware of the things that can impact this reimbursement.”
To help maximize reimbursement potential, Dr. Brault recommends that physician groups rely on statistical data such as group and provider-level metrics. A common best practice is to look at RVU data by diagnostic group, and then compare across each provider. This can help physician groups identify outliers on their team who may need extra help with documentation of their medical decision making (MDM).
A roller coaster ride for the Medicare Conversion Factor that determines total payment
The Conversion Factor (CF) is a multiplier used to calculate total Medicare reimbursement for covered services. The Medicare reimbursement formula is as follows: Total Payment = RVUs (x) Conversion Factor (x) Geographic Adjustment. And, per budget neutrality rules, CMS is required to adjust the Medicare CF based on total expected payments.
In 2021, the PFS Final Rule called for a steep decrease to the Conversion Factor – from $36.09 in 2020 to $32.41 in 2021. It was a correction of -10.2 percent, which would have been driven in large part by the increased RVUs for office based CPTs and new proposed G-codes.
However, the Omnibus Bill that passed at the end of 2020 addressed the decrease through several actions – including a 3.75% increase to all Medicare payments (through 2021), an extension of the 2 percent sequestration pause (through March 31,2021), and a delay in the implementation of the G2211 primary care add-on complexity code.
“The delay in the implementation of the add-on complexity code caused a re-calculation of the conversion factor,” explains Dr. Brault “By adding billions of dollars back onto the neutrality table, CMS was able to reset the conversion factor to a more manageable level at $34.89.”
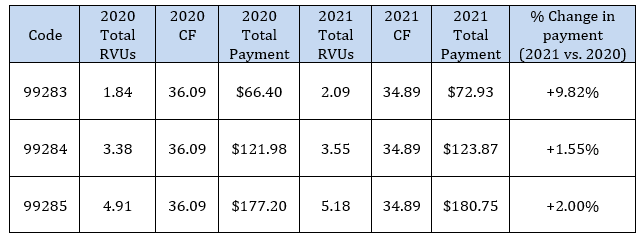
“The big takeaway here is that emergency providers will see a large increase for code 99283,” explains Dr. Brault. “However, since the beginning of the pandemic, patients with this level of injury or illness were able to obtain acute care in places other than the emergency department and this trend is predicted to continue. So, it’s likely that providers will only realize a slight increase in reimbursement as the majority of Medicare patients are expected to be 99284 and 99285 (or higher),” explains Dr. Brault.
Continuing updates to the CMS Merit-Based Incentive System (MIPS)
CMS also finalized several changes to MIPS for CY 2021, including an extension of the Extreme and Uncontrollable Circumstances (EUC) applications for COVID-19.
“Providers can now apply for a neutral MIPS reporting year in 2021,” explains Dr. Brault. “But it’s worth noting that we’re still in the transitional years of MIPS – where bonus payments are a lot easier to achieve than they will be in future years.”
Dr. Brault explains that MIPS is gradually moving away from the carrot-model of easy bonus payments and going toward the stick-model of stricter benchmarks and higher penalties. Thus, in 2022, with full MACRA implementation, a significant number of providers are at risk for a negative adjustment.
“Physician groups think should carefully about the pros and cons of taking a MIPS exception in 2021,” says Dr. Brault. “The rules of the game are still relatively easy in 2021. So, for many groups, this is the best time to refine their MIPS reporting efforts before the stakes get higher. It would be wise to use 2021 as your opportunity to build in good habits and processes.”
Learn more about upcoming MIPS changes: Preparing Providers for Full MACRA Implementation in 2022
A new CPT code for Medication Assisted Therapy (MAT).
A new CPT code was also introduced this year. Code G2213 offers new guidance for: initiation of medication for the treatment of opioid use disorder in the emergency department setting, including assessment, referral to ongoing care, and arranging access to supportive services. It’s meant to be used as an add-on code to the primary E/M services provided and/or Observation or Critical Care.
“The applicable services under this new CPT code include Initiation, Assessment, and Referrals – but the final rule doesn’t provide many details about these services,” explains Dr. Jason Adler, Vice President of Practice Improvement at Brault Practice Solutions. “However, emergency physicians have been on the front line of the opiate crisis for years and are well versed in advocating for this vulnerable population. It’s wonderful to see these programs get funding.”
Dr. Adler explains the documentation should follow medical necessity and specifically address:
- “Initiation” may include what medication was offered and for what duration.
- “Assessment” may vary based on the clinical context; there are a number of withdrawal scoring scales, opiate use assessments, and the DSM-5 criteria for Opiate Use Disorder. Medical necessity will drive this assessment.
- And, lastly, a “Referral” is always needed to complete the MAT requirements. The referral process will vary across institutions, but may include an SBIRT counselor seeing the patient in the emergency department or a discussion with written information for follow-up care.
“The value of a MAT program cannot be overstated,” says Dr. Adler. “Studies have shown that more patients engage in treatment after MAT services in the emergency department, versus a referral alone. We also know that patients who receive information about drug treatment after an overdose are more likely to seek treatment. So, it’s encouraging to see this work life saving work being recognized.”
The G2213 code is valued at 1.3 wRVU, or 1.89 total RVU’s.
New Guidance for Monoclonal Antibody Treatment
Dr. Adler explains that emergency providers should also be aware that CMS has released new reimbursement codes for monoclonal antibody treatment for COVID-19, drug infusion, and post-administration monitoring.
“The ED has become a common setting for this treatment because of logistical and other issues involved with these infusions,” explains Dr. Adler. "Groups should also be aware of programs like this that are supported through federal Covid-19 relied legislation.”
These codes are available for dates of service 11/10/2020 for Eli Lilly’s Bamlanivimab (M0239) and 11/21/2020 for Regeneron’s Casirivimab and Imdevimab (M0243). CMS has set the national average payment rate at $309.60 with adjustments based on geographic location.
Learn more about these Medicare Part B payments.
________________________________________________________________________
Article Contributors:
Dr. Andrea Brault, President and CEO at Brault Practice Solutions
Dr. Jason Adler, Vice President of Practice Improvement at Brault Practice Solutions
About Brault:
Brault is a revenue cycle and practice management organization that partners exclusively with hospitals and acute care physician groups. Their intelligent practice solutions include MIPS optimization, practice analytics, and provider documentation training. Learn more at www.Brault.us




