
Getty Images
Entering the Next Phase of Value-Based Care, Payment Reform
The healthcare industry has learned a lot from the past 10 years of payment reform for value-based care. Experts explore what the future holds for alternative payment models.

“What healthcare providers really want is to do is the right thing for their patients. They just need sustainable financial support for doing that,” health economist Mark McClellan, MD, PhD, said at the start of an interview with RevCycleIntelligence.
The healthcare industry has in earnest attempted to transform not only clinical outcomes, but also the financial aspect of care for about a decade now. Yet progress with the adoption of alternative payment models (APMs) has been slow, explained McClellan, the former CMS administrator and current Robert J. Margolis MD Professor of Business, Medicine and Policy, Fuqua School of Business.
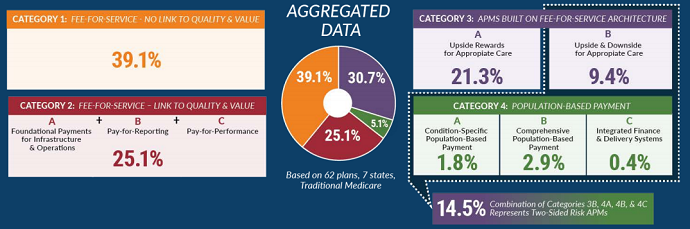
One in three healthcare payments flows through an APM, the Health Care Payment Learning & Action Network (LAN) – which McClellan also serves as co-chair for their Guiding Committee – recently found using the latest data from 62 health plans, seven fee-for-service Medicaid states, and traditional Medicare.
But fee-for-service still dominates even a decade later.
According to LAN’s data, approximately 39 percent of healthcare payments made in 2018 were under fee-for-service. Another 25 percent were fee-for-service with some link to quality and/or value. These payments included pay-for-reporting or pay-for-performance incentive payments.
The general consensus in healthcare is that fee-for-service is one of the primary reasons why the industry is sinking. The financing mechanism encourages providers to protect their bottom lines by delivering more services, which results in unnecessary costs and utilization, as well as a “sick care” system.
APMs aim to get the healthcare system back to one that incentivizes just that – health. The models tie provider reimbursement to the value of care, meaning providers get paid based on their patient outcomes and/or costs.
So, what is preventing widespread adoption of the models that promise to fix healthcare? And what needs to be done to hit the value-based tipping point? RevCycleIntelligence spoke with McClellan and other industry experts, as well as those on the frontline of value-based care, to explore the state of payment reform and strategies for progress.
The state of payment reform
The status quo is no longer working in healthcare.
National healthcare spending increased to $3.6 trillion in 2018 and is slated to reach nearly $6 trillion in the next seven years. Meanwhile, patients are not seeing the benefits of greater healthcare spending. According to data from the Kaiser Family Foundation, the US lags behind similarly wealthy countries. In some cases, such as with rates of all-cause mortality, premature death, death amenable to healthcare, and disease burden, the US is not improving as quickly as their peers.
The failings of the current healthcare system are not new to healthcare stakeholders, but there is a fresh push to fix the problems, according to Theresa Dreyer, MPH, lead of value-based care at the Association of American Medical Colleges (AAMC).
“There's a new urgency as the cost of care continues to increase to really adopt some ideas that have been existing in the market for decades and apply them to broader and broader patient groups,” she said.
Those ideas? Value-based care.
“One of the things that we see out of our teaching hospitals is a real readiness to understand that the status quo may not be the way that healthcare is provided going forward,” said Dreyer, who leads three AAMC collaboratives for teaching hospitals that participate in alternative payment models. “Many organizations see value-based care as a way of continuing to invest in the clinical changes that they are dedicated to.”
While most hospitals and physicians feel that value-based care is the right thing to do for their patients, the stakeholders are not getting on board with the vehicles being used to convey value-based care.
The data shows that the healthcare industry is about a third of the way with adopting a value-based reimbursement system. But the data does not tell the whole story, Harold D. Miller, president and CEO for the Center for Healthcare Quality and Payment Reform argued.
“We have moved backwards rather than forwards,” said Miller, a former member of the federal Physician-Focused Payment Model Technical Advisory Committee that was created by Congress to advise the HHS Secretary on the creation of APMs.
“The payment models that are being used by and large are actually making things worse rather than better in most cases,” he elaborated. “They are very problematic for patients in many cases because they create incentives to reduce spending without appropriate quality protections built into them. They are forcing many small practices and hospitals out of business.”
Physicians have been skeptical about accountable care organizations (ACOs), bundled payments, and other popular APMs. A 2018 survey of over 3,400 physicians found that many doctors (41 percent) feel value-based care and reimbursement will have a negative impact on patient care as a whole and many more (61 percent) feel the APMs will have a negative impact on their bottom lines.
Another survey published in NEJM Catalyst that same year also found that only about half of clinicians believe the alternative payment method will take off.
There is data to support their skepticism. A recent report from the non-profit Catalyst for Payment Reform showed that APMs in the commercial sector only realized small care quality improvements. Additionally, hospital readmission rates – one of the most popular care quality metrics used in APMs – barely improved under the value-based arrangements.
CMS has also expressed concerns about one of its largest APM demonstrations. According to the federal agency, the Medicare Shared Savings Program, which currently governs 517 accountable care organizations (ACOs), has actually increased Medicare spending.
“We've learned in the last few years that it's not enough just to pay a healthcare provider fee-for-service and give them a little bonus or a penalty for doing something we think we'd like them to do, like buy an electronic record system or report on a quality measure,” McClellan said.
Pay-for-performance, shared savings, and other similar APMs are a good place to start, but the models are not enough for “sustainable, effective support for truly better care models that can improve outcomes and lower costs significantly,” he added.
CMS and other major payers have started to recognize that APMs built on fee-for-service are not leading to the results they had hoped for a decade ago, and these stakeholders are refining their value-based care strategies to hold providers more accountable for outcomes as result.
Is financial risk the answer to APM progress?
“After six years of experience, the time has come to put real ‘accountability’ in accountable care organizations,” CMS Administrator Seema Verma said in 2018 after announcing the agency’s plan to revamp the Medicare Shared Savings Program.
What she meant by accountability was downside financial risk. In risk-based APMs, providers are accountable not only for the savings they achieve through the model, but also financial losses. If providers in APMs with downside financial risk exceed their spending benchmarks, they must repay a portion or all of the losses to the payer.
CMS sees financial risk as the future of value-based care, according to Dreyer. The agency believes that holding providers financially accountable for losses will result in more meaningful changes and outcomes.
However, downside financial risk may not be the key to unlocking value-based care success in APMs, industry experts contended.
“The notion that somehow if you push financial risk onto physicians or hospitals, you are going to get better quality care or lower cost is just wrong. It is an insurer view of things,” Miller said. The main issue with risk is that current APMs put providers at risk for outcomes they cannot control, he explained.
Miller pointed to APMs for oncology care as a prime example.
“The biggest cost of cancer care is drugs and one of the places where you've seen the fastest increases in drug prices has been in oncology drugs,” he said. “It doesn't do anything to promote better care to try to put physicians at risk for that. What we have seen is small oncology practices going out of business because they can't afford to actually treat their patients and the payment models don't solve that.”
Focusing the future of value-based care on risk-based APMs could also alienate many providers from the transition away from fee-for-service, Dreyer added.
“There's a risk of leaving behind organizations that are newer on the value-based care journey,” she said. “The new models are focused explicitly on organizations that already have experience and if you don't already have this experience, it'll become harder and harder to enter into the market.
If risk-based APMs are not the appropriate next step for the value-based care transition, then what is? According to McClellan, the answer lies in episode- or population-based payments.

Payment structures that align with value-based care
APMs should be less about the level of financial risk involved and more about supporting the activities and infrastructure providers need to engage with value-based care, McClellan insisted.
“What really works is giving healthcare organizations payments that are more tied to the people and the whole episodes of care that they are providing,” he said.
“Population- and episode-based payments give providers the flexibility they need to deliver care,” he explained. With the flexible payments, providers can invest “more resources into things like paying for team-based approaches to care or paying for services that aren't ‘medical’ and weren't paid for under fee-for-service models.”
“But along with that, they do have more accountability for improving quality outcomes and keeping total costs of care down,” he stressed.
Only about 5 percent of healthcare payments made in 2018 flowed through one of these models, LAN reported. And payers do not expect much growth in these types of payments. A survey of payers conducted by LAN found that payers expect the most growth in upside-only and two-sided risk APMs.

To progress with value-based care and related payment reforms, Miller suggested that the healthcare industry start with identifying a metric to improve. Successful APMs target opportunities to reduce spending or improve quality, which may include cutting spending on services with little benefit to the patient or avoiding complications of a specific treatment.
Payers and providers then need to identify changes in services, as well as barriers in the current payment system, that prevent changes in care delivery. Once stakeholders do that, they can design the APM to overcome the barriers and deliver higher-value care.
With an APM design, payers and providers must determine how to operationalize the model (i.e., create CPT/HCPCS codes and modifiers, determine patient eligibility, adjust payments for performance). Finally, stakeholders can implement the model, assess its performance, make improvements.
What sets Miller’s APM approach apart from others is his emphasis on changes in care delivery, which he believes will result in value-based care that leads to positive outcomes.
“It's not the payment model that comes first, it's the care delivery,” he said. “And you have to know what the care delivery model is in order to know how to pay for it.”
How providers are managing the transition to value-based care
The healthcare industry is not as far along the value-based care continuum as industry experts predicted a decade ago, and many believe reform is needed for current payment reform efforts. But those on the frontline of care delivery are still pushing forward with care and payment transformations in anticipation of a more advanced world.
With advancements in technology, healthcare is heading in a new direction. Community-oriented, coordinated, team-based care is now possible thanks to new and improved data sharing, consumer-facing healthcare apps, telemedicine, and other capabilities.
But fee-for-service does not align with this version of care delivery.
The right APMs can help providers develop the capabilities they need to deliver higher quality, lower cost care. For example, an ACO agreement enabled an independent primary care practice in Louisiana to get the data it needed to start performing wellness visits consistently, improve coding, advance chronic disease management, and other value-adding activities.

“That, in turn, started increasing revenue,” said full-time physician at the practice Darrin D. Menard, MD, FAAFP. “Once the dollars from savings started coming in, that helped us go further with value-based care.”
APMs have contributed to an uptick in, among many capabilities, preventative care and care management, population health management tool implementation, connected health use, and social determinants of health strategies.
But engaging with an APM to bolster care quality and lower costs is not easy for certain providers.
“It's very difficult for an independent primary care practice to enter into the world of value-based care by themselves. Value-based care by definition is team-based care,” Menard explained. “I tried for many years on my own to work with Blue Cross to increase reimbursement for value-based care and I failed over and over again.”
Gary Stuck, DO, chief medical officer at Advocate Aurora Health, knows about the benefits of size. Advocate Aurora Health is one of the largest non-profit health systems in the country, and its scale helped the health system to succeed in the Medicare Shared Saving Program, Stuck said in an interview.
But the chief medical officer attributed the health system’s $61 million in savings to more than scale.
“We use many strategies to get to that number, but the key here is that we focus on getting patients the right safe, high-quality care at the right time and the right place. We know that we can provide high quality care at a lower cost when we coordinate care across the continuum,” he said.
Specifically, the health system has invested in expanding its integrated care management and post-acute care networks to “optimize the control of chronic conditions and focus on the right level of care including a home-first mentality,” Stuck stated.
Advocate Aurora Health also partners with a platform called NowPow to address the social determinants of health, which can impact between 10 and 20 percent of outcomes.

“Our care team members use it to screen for non-clinical barriers to good health and then make referrals to programs, accessing a database of thousands of community resources to help with transportation, food banks or other services,” Stuck explained. “Then, patients can be connected to the resources that better enable them to get on the road to better health.”
Menard was able to break into this value-based world and start engaging in similar activities through an ACO, too. But his ACO was run by Aledade, which brought local primary care practices together to establish a value-based contract and help them implement value-based care.
“They gave me the tools to become successful and then having their voice with the different insurance companies,” said Menard, who eventually became the local medical director for Aledade’s Louisiana and Southeast ACO. “The ACO gave us a whole team of practices across the state that we could actually finally move the needle on value-based care in a lot of these practices.”
With access to infrastructure and resources, Menard is now part of a risk-based ACO and Track 2 of Medicare’s Comprehensive Primary Care Plus program. The practice leader plans to continue taking on risk through APMs, but he still had some suggestions for improvement.
For one, benchmarking that does not solely rely on historical expenditure data could help providers stick with APMs, he stated. Attribution could also use some improvement. When payers switch an enrollee’s primary care provider, that can knock those patients off of a small practice’s cohort of patients eligible for an APM. Additionally, new independent physicians starting out do not have the patient base necessary to engage in current APMs even if they are providing some of the best quality care around.
Current APMs may have some flaws, but providers are dedicated to continuing their journey to value-based care through the models.
“Bottom line: We have embraced value-based care as a way to deliver better health. Advocate Aurora Health will continue to pursue whatever program makes the most sense for the system and our patients,” Stuck said.
The future of payment reform
As they currently stand, APMs may not be perfect but industry experts and providers agree that value-based care is the future of healthcare. As provider organizations and payers prepare to take on more advanced APMs, the healthcare industry needs to step back and assess its progress with value-based care implementation thus far.
As Miller pointed out in his APM development guide, assessing and improving how to approach care delivery and payment reform is key. And these improvements will be critical to accelerating the transition to higher quality, lower cost care.
“We need payment reform goals that are aligned with where we'd like to get,” McClellan said, “and hopefully, by 2025 not just by 2030 or 2035.”
Dig Deeper on Value-based care and reimbursement
-
![]()
Nearly 45% of healthcare payments tied to APMs: Survey
By: Jacqueline LaPointe
-
![]()
What MAHA means for the CMS Innovation Center, APMs
By: Jacqueline LaPointe
-
![]()
Senate Finance contemplates physician payment reform
By: Jacqueline LaPointe
-
![]()
Value-Based Reimbursement Grows as Providers Take on More Risk
By: Jacqueline LaPointe



